Non-Alcoholic Fatty Liver Disease: A Whole-System Problem, Not Just a Dietary One
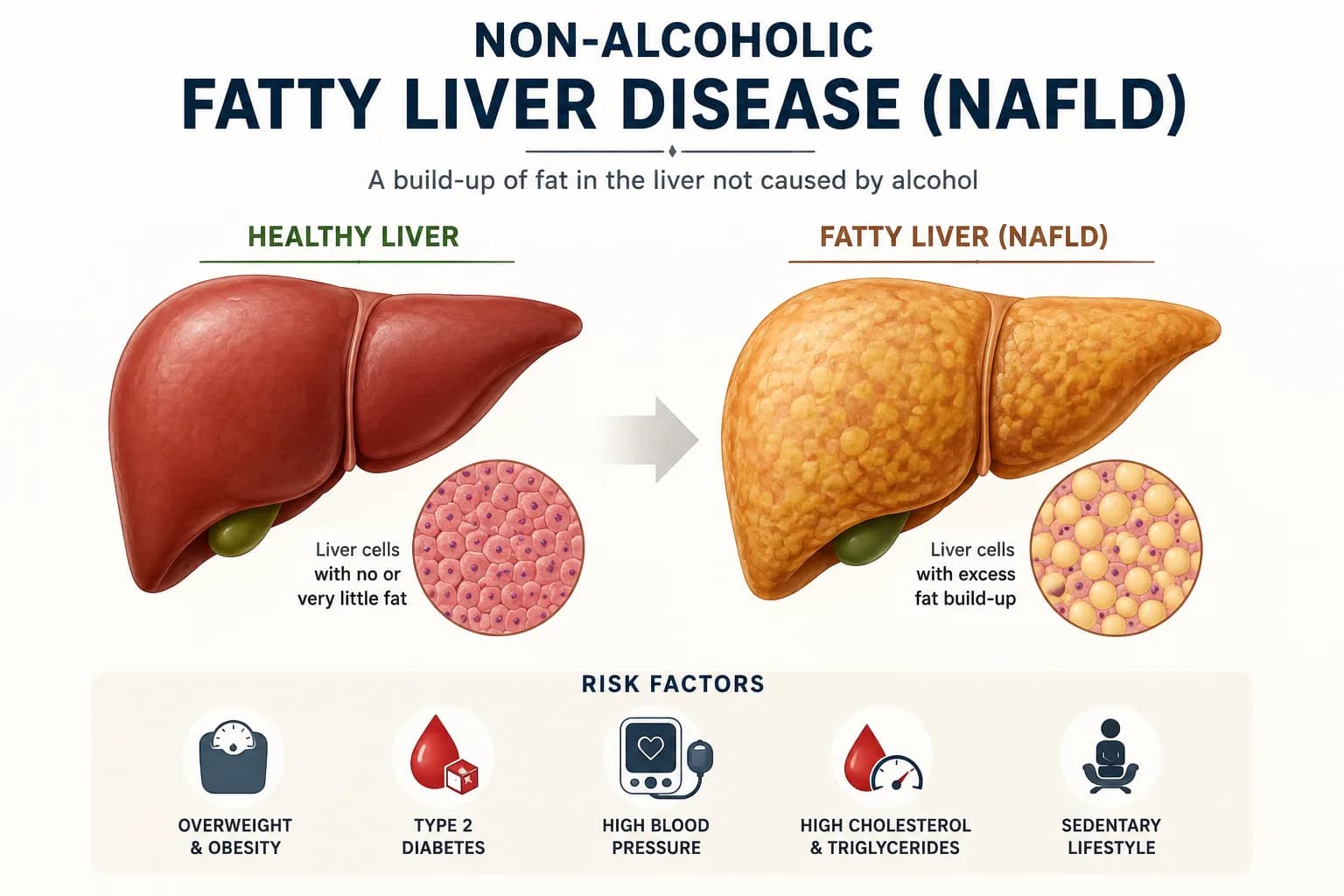
If you've been told you have a “fatty liver” — or you're worried you might — I want you to know something important straight away: this is not just about eating too much fat. Non-alcoholic fatty liver disease (NAFLD) is one of the most misunderstood conditions I see in clinic, and the name itself is part of the problem. It implies the fix is simply to eat less fat and lose some weight. The reality is far more nuanced, and far more interesting.
NAFLD now affects an estimated 1 in 3 adults in Western countries. Many people don't even know they have it — it's often picked up incidentally on a scan or through elevated liver enzymes on a blood test. Left unaddressed, it can progress silently from simple fat accumulation to inflammation, scarring, and eventually liver failure. The good news? When we understand why the liver is struggling, we have a real opportunity to support it from multiple angles — and that's exactly what I do with my clients.
Let me walk you through what's really going on.
Your Liver Is the Most Hard-Working Organ You Have
Before we dive into causes, it helps to appreciate just how much your liver is doing at any given moment. It's filtering your blood, metabolising your hormones, producing bile for digestion, regulating blood sugar, storing vitamins and minerals, and neutralising toxins. When any one of these systems starts to falter, the liver bears the burden.
NAFLD is not a single problem with a single cause. It's what happens when the liver is overwhelmed from multiple directions at once. Think of it like a kitchen with too many dishes and not enough washing up liquid — eventually, things start to pile up.
1. The Antioxidant Story: Your Liver Needs Glutathione
One of the most exciting areas of liver research right now is the role of glutathione — your body's master antioxidant, produced primarily in the liver itself.
When the liver is under stress (from excess fat, sugar, toxins, or inflammation), it generates what are known as reactive oxygen species — essentially, cellular damage in the form of unstable molecules. Glutathione is what neutralises these. Research has consistently shown that people with NAFLD have significantly depleted glutathione levels in the liver.
Here's the nuance that most people miss: glutathione is made from amino acids, and the rate-limiting ingredient appears to be glycine — a non-essential amino acid found abundantly in bone broth, collagen, and certain plant foods. Studies show that plasma glycine levels are inversely correlated with the degree of hepatic steatosis (fat in the liver). The more fat in the liver, the lower the glycine. And without glycine, the liver simply cannot make enough glutathione to mount an adequate antioxidant defence.
This is one of the reasons I offer Glutathione IV therapy in clinic — because when the liver is depleted, oral glutathione is poorly absorbed and often doesn't reach the liver in meaningful amounts. Intravenous delivery bypasses this limitation entirely and delivers the antioxidant support directly where it's needed most.
2. The Mineral Triad Nobody Talks About: Iron, Copper & Vitamin A
This is the piece of the puzzle I find most fascinating — and most overlooked.
Iron Overload in the Liver
You might be surprised to learn that excess iron is found in approximately one third of all NAFLD patients, and is so common it's been given its own name: dysmetabolic iron overload syndrome. Excess iron in the liver catalyses the formation of toxic hydroxyl radicals, which damage liver cells, drive inflammation, and worsen insulin resistance. It is a significant accelerant of liver disease progression.
But here's the important question: if iron is accumulating in the liver, why isn't the body moving it out?
Copper — The Mineral That Keeps Iron in Check
The answer often lies in copper. Your body relies on a copper-dependent enzyme called ceruloplasmin to mobilise iron out of liver cells and into circulation, where it can be safely transported and used. Without adequate copper, this iron export system breaks down, and iron begins to accumulate — oxidising, damaging, and inflaming the liver.
Research confirms that NAFLD patients with the lowest liver copper levels are the most likely to have iron overload. The two are directly linked.
Now, here's something I see regularly in clinic that is worth highlighting: many of my clients come to me already taking multiple supplements, several of which contain zinc. A multivitamin, an immune formula, a gut health product — zinc appears in all of them. But zinc and copper compete for the same absorption sites in the gut. When zinc intake is consistently high, it crowds out copper — and copper levels quietly drop over time.
This is a real and measurable problem. Someone can be eating a reasonable diet, taking what they believe to be a well-rounded supplement regime, and yet be copper deficient without ever knowing it — because nobody has tested for it. And that copper deficiency may be one piece of the puzzle keeping iron trapped in their liver.
This is exactly why I don't take a one-size-fits-all approach to supplementation, and why testing — not guessing — matters so much.
Vitamin A — Your Liver's Hidden Reserve
Your liver is the primary storage site for vitamin A in the body, held in specialised cells called hepatic stellate cells. But here's the problem: when the liver becomes inflamed and injured, these stellate cells become activated — they transform into scar-producing cells — and in doing so, they release and deplete their vitamin A stores.
Research has found a clear inverse relationship between liver retinol (vitamin A) levels and the progression of NAFLD: the more advanced the liver disease, the lower the vitamin A stores. And because vitamin A (specifically retinoic acid) is a key regulator of both glucose and lipid metabolism in the liver, this deficiency then creates a feedback loop that makes things worse.
3. Sugar Is a Bigger Problem Than Fat
Here's something that tends to surprise people: fructose — the type of sugar found in fizzy drinks, fruit juices, high-fructose corn syrup, and heavily processed foods — is one of the most potent dietary drivers of NAFLD, and it has nothing to do with fat intake.
Fructose, unlike glucose, is metabolised almost exclusively in the liver. When large amounts arrive at once, the liver converts them directly into fat through a process called de novo lipogenesis. But beyond that, fructose generates up to 100 times more reactive oxygen species than glucose, drives endoplasmic reticulum stress, worsens insulin resistance, and disrupts the gut microbiome — all at the same time.
The explosion in NAFLD prevalence since the 1980s runs in parallel with the explosion in ultra-processed food and sugar-sweetened beverage consumption. It's not a coincidence.
4. Your Gut Is Talking to Your Liver — All Day Long
The gut and liver are intimately connected via the portal vein — every single thing that gets absorbed from your gut goes directly to your liver first. So when your gut microbiome is out of balance, your liver suffers the consequences.
Gut dysbiosis — an imbalance in the community of bacteria in your digestive system — increases the permeability of the gut lining (what many people know as “leaky gut”). This allows inflammatory bacterial products, including lipopolysaccharides (LPS), to cross into the bloodstream and travel straight to the liver, triggering inflammation and accelerating NAFLD progression.
There's also the choline connection. Choline is an essential nutrient that the liver needs to package and export fat in the form of VLDL particles. Without adequate choline, fat accumulates in the liver. The problem? Certain gut bacteria actually consume dietary choline and convert it to a compound called trimethylamine — effectively stealing it before the liver ever gets it. In NAFLD patients, exactly this pattern has been observed: dysbiotic bacteria consuming the choline the liver needs.
This is why a comprehensive stool test can be such a valuable tool. Understanding the state of your gut microbiome gives us specific, actionable information — rather than guessing in the dark.
5. Hormones Matter More Than Most People Realise
NAFLD is not just a metabolic or dietary problem. It is also a hormonal one.
The Thyroid Connection
Research involving nearly 39 million individuals has shown a significant bidirectional relationship between hypothyroidism and NAFLD. People with an underactive thyroid have a 2.7-fold higher risk of developing NAFLD and NASH. The higher the TSH level, the greater the risk. Hypothyroidism raises LDL cholesterol and triglycerides, impairs fat clearance from the liver, and creates the conditions for fat accumulation and oxidative damage.
If you've been told your thyroid is “borderline” or your TSH is in the normal range but you still feel unwell — this is worth investigating more deeply.
PCOS & Cortisol
Want help making sense of your blood results? Book a one-to-one consultation tailored to your health history.
Book Consultation →For women with polycystic ovary syndrome (PCOS), the hormonal imbalance — particularly elevated insulin — drives fat into places it doesn't belong, including the liver. Research has also linked elevated cortisol (the stress hormone) to a higher likelihood of developing fatty liver. Chronic stress, poor sleep, and adrenal dysregulation are not separate from liver health — they're part of the same picture.
6. Insulin Resistance: The Central Thread
Running through almost every cause I've described above is one common denominator: insulin resistance. When cells stop responding properly to insulin, the body produces more and more of it, which drives fat storage — including in the liver. It also worsens inflammation, disrupts mineral homeostasis, and feeds the cycle of oxidative stress.
Addressing insulin resistance is often the single most impactful lever we can pull — and this doesn't always mean dramatic weight loss. Strategic dietary changes, targeted movement, sleep optimisation, and supporting the gut microbiome can all significantly improve insulin sensitivity.
One of the programmes I work with — the Feel Great system — is specifically designed to improve metabolic health and insulin resistance, and I've seen excellent results supporting clients through this alongside their personalised nutritional plan.
7. Genetics: The Hand You Were Dealt
For some people, there is a genuine genetic component. A variant in the PNPLA3 gene is the most well-studied heritable factor associated with NAFLD, and interestingly, it also affects how the liver processes and mobilises vitamin A — connecting the genetic story back to the mineral story.
Genetics doesn't mean destiny, but it does mean that some people need to be more proactive than others. Understanding your genetic predispositions — through testing such as DNAmap panels — allows us to tailor recommendations specifically to how your body works, rather than applying generic guidance.
Bringing It All Together
NAFLD is not one problem. It is a web of interconnected systems — antioxidant capacity, mineral balance, gut health, hormonal function, insulin sensitivity, and genetic susceptibility — all converging on the liver.
This is why a one-size-fits-all approach of “eat less fat, lose weight” is so inadequate. And it's why the clients I work with who make the most meaningful progress are those who take the time to understand their own picture.
Here's what a multifaceted approach can look like in practice:
- Depleted glutathione? Glutathione IV therapy plus targeted amino acid support.
- Iron accumulating, copper low? Mineral testing, a supplement audit, and strategic repletion.
- Gut dysbiosis stealing choline and driving inflammation? Comprehensive stool testing plus personalised microbiome support.
- Insulin resistance at the root? The Feel Great system alongside dietary and lifestyle strategies.
- Thyroid or hormonal drivers? Functional blood panel interpretation plus targeted support.
- Genetic predispositions? A DNAmap genetic panel plus a personalised plan.
Ready to Find Out What's Really Going On?
If you suspect you might have a fatty liver — or you've been told you do and you don't know where to start — I'd love to help you make sense of it. Your liver is incredibly resilient. With the right support, it can regenerate and recover. But it needs the right information first — and that starts with understanding your own system.
There are several ways to work with me:
Let's get to the root of it together.
Nicola Charnock DipNT, mBANT — CF Organic Wellness
This blog is written for educational purposes and does not constitute medical advice. Please consult a qualified healthcare professional before making changes to your health regime.


